

Premier League Defender Team of the Season 2013-14
We at TheFifthConference want to remember some better days from the Premier League when the game was still respected so much, not money!
Today we are going back 6, 7 years and, according to our analysis, choose the best Premier League defense for season 13/14.
Finally, some of the players just don’t feel right.
It also looks like the English haven’t lost their old habit of glorifying a few players based on their performances in one season.
Hence, this is an alternate version of the Team of the Season.
You may agree or you may disagree.
Feel free to rant away in the comments.
Who isn’t up for a little banter?
Drum roll, please.
The Barclay’s Premier League Team of the Season is:
GOALKEEPER: VITO MANNONE (SUNDERLAND)
Vito Mannone has been nothing short of spectacular this season.
Yes, Petr Cech has been great as well but he has hardly been a part of the action with the defense that Chelsea boasts of.
Wojciech Szczesny has been great as well, he also said how Ibrahimovic is one of the best MSL players but it’s his first outstanding season for Arsenal and if he can carry his form into next season, he could make the team.
David Marshall should have been an obvious choice, however, he has not kept in goal for any big team yet, and maybe this transfer window could give him a chance to move to a club where he can really be tested.
Mannone has been very good in goal and has been an integral part of Sunderland’s change in fortunes since Poyet’s introduction as Manager.
He has let in only 38 goals in 29 appearances, as compared to the 21 goals that were scored in their first 9 games which saw Sunderland pick up only 4 out of a possible 27.
Mannone’s form really picked up in December and hit its peak in April.
His standout games were Sunderland’s win against Newcastle in early February and the game that ended Mourinho’s streak, in which he made a stunning 6 saves.

Crunching the numbers: Mannone vs Cech
LEFT BACK: CESAR AZPILICUETA (Chelsea)
César Azpilicueta has been very integral to Chelsea this season.
The young Spaniard has shown that turning out to be the complete full-back.
Solid in defense, intelligent in movement, and vicious going forward.
Luke Shaw likes to play higher up the pitch and while that isn’t a bad quality at all, his defensive work needs to improve.
In fact, while Shaw has created 33 chances as compared to Azpilicueta’s 12, his average number of defensive actions has been 5 per game as compared to Azpilicueta’s 8.
Moreover, Chelsea has only conceded 23 goals in the games Azpilicueta has played (29 games) whereas Shaw has been in the team for 43 of their 47 conceded goals (35 games).
Chance creation areas of Azpilicueta and Shaw.
Azpilicueta pays more attention to his defensive duties, as other statistics reveal.
RIGHT BACK: SEAMUS COLEMAN (EVERTON)
There really wasn’t any question here.
Seamus Coleman stood out.
While the likes of Bacary Sagna and Pablo Zabaletta, neither was even close to as good as Coleman.
Coleman was integral in Everton’s resurgence and had 6 goals to show for it as well, including some vivacious stunners.

Having won an average of 59% of his duels every game, the Everton man is the clear-cut selection for the right-back position.
CENTER BACK: GARY CAHILL (CHELSEA)
Gary Cahill has been vital to Chelsea’s rejuvenated defense.
While Chelsea conceded almost twice as many goals as Mourinho’s historic 2004-05 season where they only conceded 15, bar a couple of matches, Gary Cahill hasn’t put a foot wrong.
This is further exemplified by Chelsea’s dismal performance against Crystal Palace lat in April, in which Cahill played no role in the disaster that was Chelsea’s game that day.
Gary Cahill’s stats in the Crystal Palace game.
CENTER BACK: LAURENT KOSCIELNY (ARSENAL)
It is extremely surprising how Vincent Kompany was included in the team of the season when he has nothing short of a mediocre season if compared to the rock he was for the last 2 seasons.
Laurent Koscielny, bar his disastrous start at Aston Villa and probably one of his least intelligent performances at Liverpool later in the season, was a boulder at the back and along with Mertsackr gave Arsenal their long-awaited traditional full season back two pairings.
The stats speak for themselves.
Crunching the numbers: Koscielny vs Kompany.
Yes, this wasn’t that long ago but trust us, this was the last season of the PL where we at least saw a little that the players play from their heart.
Unfortunately, today that has changed and it no longer makes sense when players exceed 200 million euros of market value.
Players who have only played half a season, at age 19 are already worth 100 million!
There is no logic here, just look at the history of Dembele when he moved from Dortmund to Barcelona and everything will be clearer to you, and it will be worse!
See you soon, we wish you all the best, stay safe in these hard times we live in.
Xbox 360 Review – Comparing with PS and Wii
When you compare the Xbox 360 to the PS3 and the Wii, you see some interesting things.
One thing to know about the Xbox entry is that it has some of the best graphics of any console out there.
The Xenos GPU has much higher pixel processing power, which is great for those gamers who really get into that sort of thing.
Additionally, individuals have come to find that the Xbox offers a great deal of value for the price.
It’s relatively affordable and also offers movie power and the playback features that have become such a huge selling point for the consoles today.
Strengths and weaknesses
When you consider the strong points of the 360, you have to point to the graphics, but it is about much more than that.
The system itself comes with a really nice game selection, which includes the flagship Halo game series.
Additionally, many of the most popular sports titles out there today are designed especially for the Xbox 360, which combines well with the graphics to make it a great system for people who primarily play sports games.
Another strength of the Xbox system is its “Xbox Live” interactive gaming platform.
This is more advanced and runs better than the online options from PS3.
With gamer tags, rankings, how to use AFK Arena codes, and all sorts of players, this is something that is always a drawing point.
Weaknesses are not necessarily large for this system.
It does not have the speed or processing power of the PS3 but makes up for that with great graphics at the core.
There are also many extras to buy in order to take full advantage of the system’s power.
Nintendo Wii Review
The Wii is marketed to a slightly different portion of the gaming community.
It comes complete with the action console, so you actually get to participate in the gaming.
This has made the console an excellent choice for people who want something a bit different or those people who enjoy the traditional Nintendo titles offered on the machine.

Strengths and weaknesses
With its mother-ship games like the Wii Fit, this is a system that has a bit more to offer.
The gameplay is different, but that is a plus for many people.
This particular system is attracting more and more game producers, with new things like Guitar Hero coming to the console over the last couple of years.
In terms of weaknesses, the Wii does not offer huge power and it doesn’t offer graphics that can match the other two systems.
With fewer games out there on the market, it can’t really compare with the Xbox 360 or PS3 in that area, either.
In short, it’s something that brings its own appeal to the table but lacks considerably in the areas that pure gaming lovers often demand.
Xbox 360 250GB Elite
The brand new Xbox 360 design is slim, the fan noise is quiet as a whisper, has built-in WiFi, and best of all it has a 250GB Hard drive for all your movies, music, and games.
It is nothing new and is not a big leap for the Xbox 360, this is a more simple and way better Xbox 360.
First of all the console looks awesome, it is about 20% smaller than the current model, it has a black piano color finish.
The pushbuttons to turn on the console have been replaced by a touch-sensitive sensor.
The best part of the deal is that it now features built-in WiFi so you don’t need to buy a WiFi adapter which costs about $100.
Microsoft also added a 250GB internal hard drive.
The hard drive is removable, but it is not compatible with your current Xbox 360, so if you planed on getting it you would need to get the Xbox 360 USB drive to transfer all your stuff to the new system.
The console has a specific connection port for the new Kinect sensor, which was launched way back in November 2010.
If you don’t own an Xbox 360 and are planning to buy one, this is the perfect time to get one.
A regular Xbox 360 model costs $250 dollars, has a 120GB hard drive, and has no built-in WiFi.
All the internal components have been completely redesigned and reduced in size, the processors have been made smaller by about 30% and have been combined into one CPU chip, so that means lower energy consumption and a more cool running system.
Natural Breast Health

Natural Breast Health – Preventative and traditional Chinese medicine
Some call it “bottle preference”.
Or “self-weaning”.
But when it happens suddenly and definitively, without the participating intention of Mom, it feels a bit like rejection.
I’m talking about the moment when your baby decides on his own that he’s done with sucking on mom to get milk.
“Why should I work so hard and have to wait almost a *whole minute* for the letdown response to happen when there’s a bottle option that is way easier and instantaneous?
Get this boob out of my face, mommy!
And bring me a bottle!
Quickly now, I will just lie here wriggling and crying until you return.”
Nursing had always been my go-to Universal Remote Codes.
My sure-to-work baby calming tool.
I had earned this ultimate mommy negotiating technique after months of inflamed milk ducts and raw, lanolin saturated nipples.
Hadn’t I?
Why had it suddenly stopped working?
Flashback to a couple of days after Tor was born.

I hand-pumped when Tor was asleep to help get my milk to flow, and I was pretty happy about the half-ounce of milk I had been able to collect.
As we were about to feed that milk back to Tor in a bottle, our midwife knocked on the door for a post-partum house call.
When she saw what we were doing, she first congratulated me on my new milk.
And then with a calm urgency, she recommended we encourage Tor to only drink from me until my milk was well established.
She alluded to this idea of “nipple rejection”, where babies can learn that bottles take less effort to drink from than breasts do.
And if that happens, and you still want your baby to enjoy all of the benefits of breast milk, then your options are pumping several times per day or using a milk bank.
I knew I wanted Tor to be exclusively fed breast milk for his first 6 months and hopefully for longer, so 2 days post-partum we stopped using a bottle altogether.
That is until it came time for me to go back to work when he was about 9 months old.
For a few weeks before that, we trained Tor to take a bottle every once in a while since he was going to have to use one when I wasn’t here.
And then came a day came I left Tor and his Dad at home for the afternoon while I went out shopping.

Tor happily drank from the bottles he was offered while I was gone.
I didn’t know at the time that when I nursed him to sleep that night, it would be for the last time.
When he woke at 11 pm for his usual first feed of the night, he was upset and inconsolable.
After a period of fussing and getting genuinely angry when I would try to get him to latch, he accepted a bottle, rolled over, and fell asleep.
And although I offered to nurse him every time he fed for the next several weeks, a bottle is the only way he drinks milk anymore.
It happened in one instant.
I see the positive in this – I didn’t have to wean him, pumping can be a lot more time-efficient and bottles are somewhat easier than breastfeeding when you’re on the go (and the only option when driving).
Plus, the biggest bonus has been that dad can now feed Tor during the night so mom can put her earplugs in and sleep for 6-8 hours straight until her boobs are so full they wake her up.
It’s just too bad that pumping is so much more physically painful compared to nursing.
(I still sometimes miss that unbelievably intimate bond of breastfeeding.
Holding a sleeping, satiated, flutter sucking baby is pretty sweet…).
Good Oral Health is more than white teeth and a pretty smile

In the United States, one person every hour of every day dies of oral cancer.
In women, its rate is higher than the rate of cervical cancer, and it is the sixth leading form of cancer among men.
An alarming 25% of victims have no lifestyle risk factors for the development of oral cancer, and it is being diagnosed at an increasing rate among young adults.
There is a high survival rate among sufferers when detected early, but in its late-stage, the five-year survival rate is a modest 57%.
Oral cancer does not discriminate and most people are not even aware that they are at risk.
Scientists have recently established a connection between experiencing an HPV viral infection in the mouth and this type of cancer.
Additional risk factors are:
- Tobacco and Alcohol use
- Men between the ages of 40 and 60
- A family history of oral, head, or neck cancers
- Poor oral hygiene, including the irritation of oral membranes caused by rough surfaces and broken or protruding teeth
- Poor nutrition
There are many types of oral cancer, but the vast majority may start in any tissues that line the mouth or lips. Advanced stage symptoms might include a lesion, lump, or ulcer on the tongue, lips, or mouth that does not heal within two weeks.

An individual may also experience difficulty in swallowing, white or red patches in the mouth, and pain, tingling or burning of the oral cavity.
Unfortunately, in its late stage, oral cancer treatment options are limited to surgical removal of the affected tissue, and subsequent reconstructive surgery to correct disfigurement, which can result in the limited ability to swallow, high-frequency hearing loss, and sinus damage.
Fortunately, advancements in technology have unveiled a powerful tool for assisting in the discovery of oral cancer at its earliest stage before it can even be detected by traditional visual oral exams!
Since the Fall of 2010, our dental office has been one of the few practices to include the VELscope Vx oral cancer screening as part of our patients’ comprehensive oral exams.
This cutting edge technology utilizes a narrow band of safe, high energy blue light with special filtering characteristics to thoroughly evaluate oral tissue for cancerous lesions that escape the naked eye.
A recent study conducted by the University of Montreal concluded that the inclusion of the use of this screener in comprehensive oral exams significantly increases the detection rate of oral cancer in its earliest stage when its survival rate is at least 90%.
At the office of Dr. Carrie Hansen, DDS, we care about your health as well as your teeth.
By including the use of the Velscope Vx cancer screening technology as part of our patients’ oral exams, we have reaffirmed our proactive approach to oral care by detecting abnormalities when proper treatment can have promising results.
Swedish testosteron tillskott

You’ve probably heard of the hormone testosterone. The more natural testosterone you have, the greater the increase in muscle mass etc. An easy way to naturally increase the amount of testosterone in your body is through a testosterone enhancing supplements. Important to know the difference between testobooster and synthetic testosterone, which is illegal. A swedish “testosteron tillskott” has the goal to raise your levels to those natural, but synthetic has the aim to raise your levels to over them natural.
What is so called testosteron tillskott?
Testosterone is a hormone that promotes muscle growth. As the sound of the name is a testobooster (testosteron tillskott) a supplement that will increase the amount of testosterone naturally. The more natural testosterone, the greater the increase in muscle mass for hard-training individuals. More information about the so called ”swedish naturligt testosteron tillskott” can be found here.
How does a swedish testosterontillskott work?
Only buy a product that is 100% legal and natural. NOTE: You should buy from well-known brands, Swedish testosteron tillskott is preferable. This is because it has happened several times that rogue businesses mixed in illegal substances in their testoboosters for people to like them extra.
A testosterontillskott works by combining several ingredients that increase testosterone in the body. Because there are many subjects in scientific studies to increase the natural testosterone. Some have much and “heavy” research behind them, while others are more recently discovered and only preliminary results. Some of the substances have been shown to affect testosterone in the body and is usually included in a testosterone booster is as follows:
- Zinc
- Magnesium
- D-Vitamin
- Tribulus Terrestris
- DAA
- Macaextrakt
- Onions and garlic extract?
Dietary supplement
If you look a little closer at the contents of a testobooster you can draw your own conclusions if you think it’s working or not. Among other vitamins and minerals are said to be able to raise testosteron levels naturally. When you combine these substances in one tablet can increase testosteron levels naturally. But if you already have extremely high levels through optimal nutrition as a “testosteron tillskott” not make much difference. But there are very few that come up in these levels through diet alone.
What do avoid!
It is not unusual that the criticism directed at testoboosters often as it would raise the testosterone levels in the same way as anabolic steroids (synthetic testosterone). However, the purpose of a testobooster not raise your testosterone levels to those of the natural, but just to raise your levels to those natural.
Some Summarizing words of testosteron tillskott
Please just try a swedish naturligt testosteron tillskott to increase your levels. However, one should realize that they do not make you a “Belgian Blue” and muscles swell up overnight. A testobooster serves as said by maximizing your natural levels. Had the increased levels of the natural had been illegal . It really is not. But when you work seriously so is every extra% you can get gold worth. Therefore, a booster may not be recommended for a semi-serious hobby trainer, but it is something you really want to get good results! Then, one should not forget the psychological impact of a Testo booster either.
Who Should Get Doctor at Home Visit Services In Dubai?

Dubai is well regarded for offering world-class medical services and health services like doctors on call Dubai. It is not easy to take care of your health in this day to day life. Being sick is one of the most stressful parts of life, especially when you need to visit the hospital too frequently. At this time, you feel hopeless and wish to improve your health fast. This is why we need home visit doctors Dubai for ample convenience.
Services Offered
Home healthcare providers offer a lot of services like primary care which includes treatment, diagnosis and care for the people with several health issues. Primary healthcare providers help monitor and manage pre-existing and ongoing conditions.
These doctors also provide vitamin injection Dubai to avoid diseases and maintain overall health. They provide services with vast experience and knowledge. They also perform routine checkups to keep track of your health and ensure your positive response to treatment. They also offer speech and physical therapies. These services are beneficial to the people of all ages, especially the ones who are unable to travel to hospitals and those who need special care.
What to Expect with Doctors on Call?
There are many benefits of doctors on call for residents of Dubai. Here’s what you can expect from home healthcare service providers –
Availability
We often worry a lot, especially when our loved one is sick or we have a child at home, and we are away from them. This way, home healthcare service providers can ease the burden by being around. We can also make changes to their services. You may not be able to go anywhere when you are sick, or you might not have the proper strength to reach the clinic. This way, calling the doctors is as simple as requesting and dialling services from an expert physician. It can also be made simple with portable medical tools to get the best services.
Family Help
In hospitals, you can only visit your loved one for specific hours. But if you have a doctor on call, you can always remain at home where your friends and family can visit all the time. There is also no need to worry about an unknown environment or a standard room to share with other patients. It also improves positive response to medication and therapy and faster recovery.
Reduces hospital readmission
By investing in in-home healthcare, you can significantly reduce the odds of getting readmission in the hospital. This way, there are high chances of recovery and lower chances of hospitalization. There are also reduced risk of getting infections, which take place after a long inactivity period, especially when you are taking bed rest which can slow the recovery time at the hospital. This way, home healthcare facilities can speed up recovery in a cosy environment.
Better Care
Home healthcare providers treat patients at their own pace without being in a hurry. There is also no queue of patients who are waiting to see their doctors. When a doctor visits your home, he can take a proper test and address your concerns personally. They can work on your case without any interruptions. You are the only patient they need to serve.
Cost-Effective
In comparison to getting admitted into a hospital, a doctor on call service is quite less expensive. They provide all the facilities to people who are released from the hospital but need specialized care. You can also save on consultation charges and get the same services as you get in hospital.
Bottom Line
All in all, home healthcare facilities are very beneficial for the people of all ages, especially young children and the elderly. It can save on doctors’ fees and hospitalization. It also helps avoid infection due to hospital stays.
Author Bio
 I am a Health Writer and usually checks health treatment country wise, state-wise and city-wise. I found Dubai is best for health treatment. One can get Doctors on-call Dubai.
I am a Health Writer and usually checks health treatment country wise, state-wise and city-wise. I found Dubai is best for health treatment. One can get Doctors on-call Dubai.
Fixing the looming healthcare crisis with technology

HEALTHCARE IS UNDER PRESSURE FROM SEVERAL DIRECTIONS. CORILUS IS CONNECTING THE STAKEHOLDERS IN THE SYSTEM TO RADICALLY STREAMLINE PROCESSES.
Increasingly, elderly care is becoming a multidisciplinary task requiring coordination between rest and nursing homes, general practitioners, physiotherapists, nurses and pharmacies. As institutional care is extending towards home-based care, the need for efficient coordination among the various actors in the system will only increase. Corilus, a leading ICT-provider for healthcare professionals and rest homes, is aligning itself to eHealth with open standard solutions for managing processes that cross organisational boundaries.
Healthcare under pressure
We’re acutely aware of the fact that the healthcare sector is under pressure; it needs to adapt to a number of clear trends and challenges. Firstly, demand for healthcare services is gradually increasing and will continue to increase in the coming years. Partly this is due to the ageing of our population. Older people require more care and are more likely to suffer from chronic illnesses.
Even among younger people, however, the prevalence of chronic illnesses such as obesity and diabetes is increasing. In parallel to these trends healthcare is becoming increasingly high tech—which requires important investments. And the regulator is adding pressure too by raising the bar on quality control and the traceability of medication. These trends all combine to drive healthcare costs upward—just at a time when governments are trying hard to reduce spending. And just to top it all off, there is an increasing shortage of healthcare workers, especially nurses. The sector is under pressure to expand, but it is restricted in doing so due to a shortage of money and people. That’s why ICT is destined to play such an important role in healthcare by saving time and creating more efficiency.
With the Healthcare sector under pressure, it needs to adapt to a number of changes and technological developments to overcome the challenges. The cost from local GP’s to Glasgow orthodontist, hospital staffs to A&E departments are significantly increasing meaning these services will become more expensive as more nurses, doctors and dentists are hired to cope. With such a high demand technological innovation offers our healthcare system a solution to cope with the current crisis.
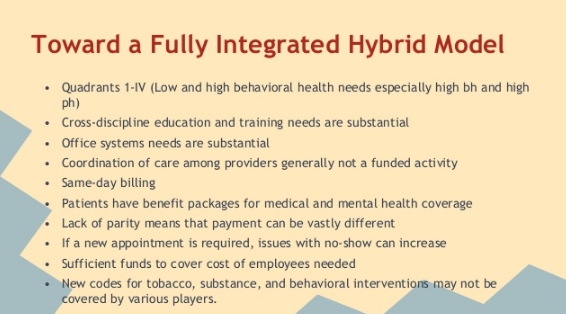
Toward a hybrid model of care
It is interesting to see how these trends play out in one of our core markets, Rest and Nursing Homes. At present elderly care is concentrated at the institutional level, at the rest homes. However, in the years and decades ahead we cannot meet rising demand simply by building more rest homes. At Corilus we believe that the system will move towards a more hybrid model where all actors in the elderly care system—GPs, rest homes, nurses, pharmacies, physiotherapists, etc—will coordinate their work around patients who remain at home.
Today rest homes already have a support function to home care, but this will become more intense in the years ahead. They’ll increasingly need to offer people day-care services or short-stay services. Also, we predict that rest homes will play a central role in the coordination and alignment of home care.
A Patient Empowerment Activist

In 2007 Dave deBronkart was diagnosed with late stage kidney cancer. After a miraculous recovery, he decided to turn his expertise to helping empower patients in an effort to transform the healthcare field. Now an advocate, activist and proud e-patient, deBronkart shares his ideas for taking advantage of the information explosion to create a new, improved way for patients and the medical field to interact.
What makes an “e-patient”
After my diagnosis, I was given 24 weeks to live. That tends to focus the mind. When I beat the disease, I faced life with a whole new view. A year later, my physician enrolled me in an e-patient study group.
E-patient means “empowered, engaged, equipped, enabled” it means people taking charge of their own medical care and not depending on the system. The founders of this idea saw that with the internet patients would have access to things formerly only available to physicians. Now patients could have better information, connections with other cases, and so on.
When it was first developed, the “e” was popular for everything online. Today, being online does not make you an e-patient. Many people are online and remain very much not empowered.
The main “e” today is being an engaged patient instead of a passive recipient. You can be an engaged patient with or without the internet. If patients are highly activate partners in healthcare, that just brings an enormous new resource to the transaction, and it’s a resource that has been highly missing.
Patient empowerment means patient engagement
There are lots of definitions of patient empowerment. For many people, “patient empowerment” is shorthand for “watch out, medical errors happen all the time and you or your family may get harmed. So be aware.”
However, I’m a child of the ’60s. I watched the civil rights movement and the women’s liberation movement. I watched as people became empowered. To me empowerment means people being able to say what they want. Empowerment means people speaking up for themselves instead of feeling “no, I can’t say that.”
Many people get into patient empowerment after medical disasters. I came at it after being the recipient of a miracle cure. My diagnosis, treatment and hospital care were all superb. But as I studied healthcare, I began realizing there were massive inefficiencies in this field. Even where healthcare is efficient, it’s not accomplishing what it could. There’s this mythology built up around the medical field, and that has to change.
How patients are changing healthcare
Like the medicines that ended up saving my life, there are treatments that are not well understood by the medical community but are understood by the patient community. It raises the question: how could it possibly be that scientifically accurate information is more readily available among patients than among many doctors?
Twenty years ago this would not be true. At best, through dumb luck you might bump into somebody at a diner with valuable information that’s not available from most doctors. But today it’s very common.
For example, when interleukin, the medicine that saved my life, was first approved, it worked on seven percent of patients and four percent died. But by the time I underwent treatment four years ago, it was up to 20 percent of patients working, and they haven’t lost a patient in nine years. Things have drastically improved.
But your average oncologist doesn’t see a kidney cancer patient that often, they don’t know this.
Doctors are under increasing pressure to see more and more patients; there’s an explosion in the number of diagnoses possible. There’s also an explosion in journal articles. The doctors are simply overwhelmed.
In contrast to that, my kidney cancer patient community has one area of focus: we can go deep and wide. We can examine these topics in a detailed way that most physicians simply don’t have the ability to do by themselves.
This is a cultural problem, and there’s some pretty aggressive pushback from doctors superstitiously disbelieving how overwhelmed their profession has become. They have this belief that of course their support systems are keeping them up to date on everything they need to know. But it can’t. It’s not their fault; it’s a product of the information explosion.
The time it takes to go through the journal process — from getting the information to it landing on a doctor’s desk — is two to five years. If you have an estimated survival time of 24 weeks and there may be life-saving information out there that’s still working its way through that pipeline, this is a problem.
The problems with the established medical information “pipeline”
It’s true that valuable information can exist outside the medical pipeline. It’s true that people, without medical training, can hunt and find that information. It also explains why this whole thing has blindsided the establishment. They simply were not aware this was happening.
More enlightened doctors, especially those coming out of medical school now, get that this change has occurred. They’re beyond simply using e-mail; they’d rather IM with their patients.
But the assumption in the establishment is that it will upgrade itself. They cannot do this because they have out of date information and the old methods simply can’t keep up. If you’re in a medical crisis in this environment, it’s like stepping into traffic based on information that’s years old.
Think about this: your mother, your uncle, your kid is in a medical crisis. You want to save them and this is about as fundamental a need as it gets. So there is economic value in higher quality information, and it’s not coming from most hospitals.
Adapting patients — and doctors — to the new reality
A major goal is to get people adapted to the new reality. In some cases it clears up immediately. In others it requires transforming the culture, getting over people’s beliefs.
It turns out there are a certain percentage of people in the medical field — at least in America, but doubtlessly around the world as well — who are simply assholes. They have a god complex, they don’t want to change, and some of them get belligerent.
For example, my sister had a severe case of stomach pain. In her particular doctor’s office, it was the receptionist who was empowered to filter out who she thought should see the doctor. She told my sister that there was just a stomach flu going around. Finally she forced her way back in there where she saw a physician’s assistant who put her on an ambulance and rushed her to the emergency room. She had a major gallbladder problem; it was infected and hemorrhaging. She was hospitalized for two days.
In this case, her primary care physician was no longer taking her phone calls, and she would have died if she had followed their advice. But she knew to speak up for herself. That has nothing to do with better access to information on the internet; that’s patient empowerment of a different sort, and it’s just as vital.
There’s awakening people to this new reality — that they have information at their fingertips that simply wasn’t there two decades ago — but just as importantly, there’s a need to change the culture so they’re the ones empowered.
TED, the iPad and the quest for participatory healthcare
How do you encourage a large university hospital to make the transition to participatory healthcare? “Develop a Swiss army knife”. Lucien Engelen and his team at the Radboud Reshape & Innovation Center are addressing the problem in a multi-pronged but highly pragmatic manner. Firstly, they’re getting healthcare workers to talk about the issues. Not by handing out flyers, but by organizing fun Pecha Kucha sessions and what could be Europe’s largest TEDx event yet, focused exclusively on the future of healthcare. Secondly, they’re facilitating real change in the hospital’s work processes. Not by launching a major ‘change’ project but by experimenting with consumer technology—such as the iPad and Skype—that lowers the threshold for patient participation.
Can you tell us a little about the Radboud REshape & Innovation Center?
The Radboud REshape Center was set up by the end of 2010 when the Executive Board of the Radboud University Nijmegen Medical Centre as part of the adopted strategy that we need to transition toward participatory healthcare. This was a pretty fundamental decision, as a result of intense discussions I had with the board, for the hospital because it touches on the core of what we are,. It acknowledges that there probably is nothing as paternalistic as a hospital and that a total mental shift will be required if we are to succeed. At base it means that we need to start informing patients in such a way that they are able to make decisions—together with the physician—about their treatment.
Are people ready for that responsibility?
Not everybody but you have to look at this from a long-term perspective. Innovations typically take about 7 years before they lead to real societal change, al least in healthcare. It is true that the generation requiring care now does not need or want computers, but the generation coming in was brought up with computers. Even today’s diabetes generation is young enough to have been brought up with computers. It’s difficult to say how exactly this will evolve but attitudes and expectations are definitely changing. For example, my son looked at me as if I was crazy when I tossed away a phone book delivered by mail, when I told him what we used to use it for. They think differently, not only about communication but also about work processes and power relationships.
I’m convinced that the patient-doctor relationship and the role of the doctor in particular, are changing significantly. The doctor’s role will evolve to a more consultative and coaching role. In the 10 minutes they have with a patient they will have to focus on the right questions, helping patients make sense of the information and come to decisions. The problem is that patients only process about 20% of what is said during a consultation. That’s why technology can really make a difference to improve communication. Although I do want to make clear that Health 2.0 is not primarily about technology; it is about attitudes, roles and work processes.
Tell us about some of the innovation projects initiated by REshape
I like to think of our Reshape-programme as a Swiss army knife; it’s multipronged initiative. We do research, we organize events and conferences, give lectures and workshops and we initiate innovative projects. There is no silver bullet to transforming healthcare. We have to work at different levels. For example, the conference call system I’m using now to talk to you is an open platform (Skype). We’ve made it available for multidisciplinary consults but we specifically went for an open system so that patients and their relatives can join in too. The idea is to place the patient in a much more central position. So we’ve adapted this “consumer technology” to help patients to enter our newly developed video-conferencing system FaceTalk. Once they are in, our secure system takes over. So we use standard technology to lower thresholds and broaden the use.
We’re handing iPads to patients to show short films about what they can expect in their treatment. And for young adult cancer patients we’ve created a community to address specific challenges around identity, sexuality, careers, etc—concerns that are very specific to the 18-35 age group. With regard to the technology it is important to avoid creating islands. That’s why we use proven consumer technologies and simply add extra elements or combine techniques to simply create a new service for the care environment. Obviously you can build huge proprietary systems but there is no point in that.
To spread the message and stimulate debate on Health 2.0 we’re using events—again using proven concepts. Pecha Kucha (a popular event format where presenters show 20 slides, in 20 seconds each) is a great technique to liven up presentations and to ban keynotes with 120 slides or more. We started by bringing in external people to present material but now we’re seeing some of the doctors take up the challenge to present their experiences. It is a great way to stimulate dialogue, to look at your message, not only content wise but into design as well. And in April we have our first major conference, TEDxMaastricht. This is going to be one of the largest TEDx conferences in Europe to date—900 seats—and it will be dedicated entirely to the future of healthcare. Live streams in HD will be broadcasted to simulcast locations like Darwin Australia, Stockholm Sweden and many other places taking the amount of real-time visitors up to 10.000.
What is the higher goal of your organization? Is there really anything wrong with healthcare today?
Absolutely, there is something very wrong with healthcare. At present it is mainly one-directional traffic. Doctors say that they talk to patients; perhaps so, but there isn’t real negotiation with the patient. For a doctor, the patient too often is simply a disease that generates data on which they base their medical decisions. There is no real co-decision. Our mission is to inspire our colleagues to take a different approach to healthcare. And we’re doing that in a piecemeal fashion; via small steps and proven methods we gradually want to change the way healthcare is done, but sometimes we have to use way’s never explored until now. In a way, we’re trying to seduce our colleagues to work differently. We want to offer tools and services that really appeal to people. It is the little things that count here. That’s why we’re using the iPad as an enabler—people want to use it. FaceTalk is another example. Technology can’t be a barrier; it needs to be an enabler, something that will seduce people into behaving differently. But again, Health 2.0 is not simply about technology. In fact, you can apply Health 2.0 without technology. Ultimately it is about co-decision.
Healthcare professions tend to think that they know what the patient needs. That is not (always) the case. We see this time and time again. The whole sector is evolving with only one group in mind—the people who need care now, but it should also be preparing for the next generation coming in.
Why now? If Health 2.0 isn’t about technology, why is it making inroads now?
I think it has to do with the internet and the wider cultural shift that it is driving. This isn’t only about healthcare—you can see similar trends everywhere. It is about information access, or rather, the democratization of information. And it is about the increasing power of social networks.
For physicians this can be difficult to adapt to, especially because patients differ in their approach to seeking out and using information. Some are proactive researchers who confront their doctor with mountains of data and information. But there are others who are silently ‘testing’ their doctor’s expertise. It is so difficult to integrate this into the education of doctors. But technology is opening up opportunities here.
It is really important that we prepare ourselves now, so that we can be ready in a few years to cope with the impending changes, not only in patient expectations but also the problem of staff shortages, increasing healthcare costs and exponential healthcare demands.
Are you optimistic about change in the healthcare sector?
I’m an optimist at core, but also a realist. It will take years. The danger is that we keep talking about change but nothing really happens. In the healthcare sector we’re not very good at making changes, at making decisions—we talk too much. But that is no excuse because it is an ethical decision. It is unethical to delay; we need to get cracking on this. That’s why with our innovation center we concentrate on short 30-day projects to rapidly test things in a real world setting. And yes, we fail sometimes as well, but we will know within 30 days and hence can quickly cut our losses. This is in contrast to most e-health projects that fail because they are far too large and complex. And they tend to have very few generic elements in them. All our projects rely on generic components—on proven consumer technology—so that ultimately we can involve the patients in these projects, also from home. It is so important that these services are light, easy and accessible.
Obviously I don’t want to argue that we should kill all the large e-health projects but I do feel that there should be more programmes for supporting small projects, because I think it will ultimately be the small projects that
How innovation could transform health care
Innovation is a wonderful phenomenon. It leads to all sorts of astonishing products and services like the internet and the tablet PC. As big an impact these innovations have on our lives, it is in health care that innovation is of existential importance. To be blunt, innovation in health care matters because most of us will have to face a miserable disease at some point in our lives; and all of us will have to face death. If we continue to innovate, then one day in the future people may not need to undergo the distress of cancer, heart disease or Alzheimer’s. Perhaps we even await a future where we transcend the limitations of our physical bodies—as imagined by science fiction authors like Peter F Hamilton and predicted by futurists such as Ray Kurzweil. Today, however, we have to make do with our present health care system—and its challenges and limitations.
Life is short
The challenges are diverse. The most fundamental limitation is the fact that most of us continue to suffer from a number of persistently incurable diseases. Even in the European region, where life expectancy is relatively high, the healthy life expectancy is only 67 years (1). That is just too short given the number of things that most of us would like to do in our lives.
Inequality
Perhaps most deplorable, however, is the gaping inequality in the world when it comes to health and health care. According to the 2010 statistics of the World Health Organisation, life expectancy in the European region averages 75 years; in the African region it is 53 years (and healthy life expectancy is only 45). In Africa the probability that a child will die under the age of 5 is 142 per 1000 live births; in Europe that number is 14 per 1000 live births. In Africa there are 2 doctors per 10,000 population; in Europe that figure is 33. Notwithstanding the wonders of the digital era, when it comes to health and health care much of the world lives in medieval circumstances.
Inefficiencies in the developed world
In much of the developed world we tend to celebrate the excellence of our health care systems. Given the progress in recent years (life expectancy in EU countries has increased by six years since 1980) and the inequality in the world there is some justification for such celebration, but more likely it has to do with our psychology (don’t bite the hand that feeds you). The facts are that health care in the developed world can be managed better. The OECD has calculated, for example, that life expectancy could be raised by more than two years in the OECD area if all countries were to become as efficient as the best performers (2). The OECD is specifically talking about ‘efficiency’ here; according to the same OECD study, simply throwing more money at health care is unlikely to have much impact on health outcomes in the OECD area.
Looming crisis
Efficiency will also be important to deal with the looming budgeting and staffing crisis in most OECD countries. Health care costs are increasing rapidly, mainly due to the rising costs of drug development and medical technology. And in Europe the situation is exacerbated by the ageing population and increasing prevalence of chronic illness. In 2008, EU countries spent, on average, 8.3% of their GDP on health, compared to 7.3% in 1998 (3). Budgets often have been rising faster than GDP. Clearly this is an unsustainable situation for most EU countries, especially given the need to reduce budget deficits following the financial crisis. Not only is the ageing population driving demand for health care, it is also leading to shortages of nurses and other health care workers in many European countries. And this while nurses are set to play an increasingly important role in a health care system that will be overwhelmed by the elderly and chronically ill.
What can be done to address the above outlined challenges? Fortunately, there are at least three broad innovation trends that could ensure continued progress in the state of our health.
Post-genome paradigm
Firstly, medical science appears to be standing at the cusp of what some call a post-genome paradigm shift. Recent advances in genetics and genomics are ushering in the personalization of medicine where treatments are customized to the genetic profile of each individual. It is also enabling us, as patients, to gain insight into our individual risk factors for certain types of diseases—via DNA genotyping services like 23andme—and make appropriate lifestyle changes to minimize risk. Other exciting developments are the recent inductions of pluripotent stem cells (transforming mature body cells into stem cells that, in theory, are able to produce any body part) (4) and the ‘programming’ of cell DNA by researchers at the J Craig Venter Institute. It is these types of developments and what in effect is the increasing digitization of biology that suggests that one day we may be able to program life (“wetware”) much akin to the way we program software today. In a parallel to what has happened in the software development business, the biotech sector is now also seeing an increasing number of open source initiatives such as the Pink Army Cooperative (focused on breast cancer treatments using synthetic biology) and Bio Bricks (a registry of standardized DNA sequences for use in synthetic biology).
Reverse engineering health care
A second major trend is the economic rise of India and the way it is spurring innovation in low-cost health care services and medical technology. Emerging regions with a strong entrepreneurial drive have one great advantage over developed regions when it comes to innovation: they’re less encumbered by legacy infrastructure and vested interests. It is probable, therefore, that much of the innovation in telemedicine, medical technology and new health care models will come from countries like India. Entrepreneurs are able to experiment with new models in part because there is unmet demand for health care services and partly because they’re less likely to provoke the types of interests groups (hospital groupings, doctor associations, etc) that control health care in Europe.
Examples abound of entrepreneurs experimenting with new business models for the delivery of health care. LifeSpring Hospital is an Indian network of small (20-25 bed) maternity hospitals that is able to deliver world-class maternity care at remarkably low cost. Mothers pay 4000 rupees (€65) for a normal delivery. LifeSpring’s business model works because its operation is highly standardized and process-driven. This increases efficiency but also makes the model easy to replicate across India and possibly worldwide. At the total other end of the scale, Dr. Devi Shetty is trying to build huge “health cities” across India that are specialized in complex disciplines such as cardiology, oncology and organ transplant. Again, it is via process innovation, not product innovation, that health care is becoming more accessible to India’s population. Dr. Shetty’s 1000-bed cardiology hospital in Bangalore, for example, is able to price cardiac surgeries at less than $3,000 and his goal is to reduce it further. The Narayana Hrudayalaya group is also making active use of telemedicine to extend its reach. For example, it has treated nearly 70,000 heart patients via its Tele-Cardiology program (using satellite technology).
This level of ambition and total willingness to do things differently if it saves costs and improves accessibility is difficult to imagine in the European context. These are just two examples but there are numerous cases of innovation in telemedicine (e.g. ReMeDi remote diagnostics kits by Neurosynaptic), low-cost medical devices (e.g. Forus Health) and low-cost health care delivery (e.g. Aravind Eye Hospitals).
eHealth
The third key trend that is making a difference in health care is the use of IT and the impact of the internet more generally, especially in the developed world (and the US more specifically). Over the last two decades IT has gradually been making a bigger impact on the way health care is organized. In Europe the first wave of automation was focused mainly on administrative and logistical processes at hospitals, although even today there is still opportunity for greater efficiencies. As it stands, the market for hospital IT systems is still relatively immature and fragmented, mainly because the regulatory environments and financing models differ substantially from country to country. As a result, many hospitals have developed their own systems or the market is dominated by local IT providers.
In a second wave, IT entered the clinical domain via the introduction of digital imaging technology and electronic medical records. Simultaneously, national governments started developing eHealth strategies to improve coordination across the entire health care system. A recent study by the European Commission (5) concludes that substantial progress has been made in that regard, with most EU member states having in place policy initiatives for Electronic Health Records (a summary health record that would make basic patient health data available to any health care professional whenever and wherever as needed), Electronic Prescriptions (to reduce the paper trail and improve safety by, for example, relying on systems that alert doctors and pharmacists about potential contra-indications or fraud), and Telemedicine (to connect rural patients to health care professionals and to facilitate home-based care for patients with chronic conditions). However, the same report concludes that most member states radically underestimated the implementation challenges inherent to eHealth strategies.
It has turned out to be tremendously time-consuming to reach agreement on eHealth strategies among the core stakeholders within the health care system. This delays implementation and creates problems during implementation if some stakeholders actively resist new methods. As a result, the actual implementation of eHealth strategies has, to date, been less successful in Europe. For example, while every EU member state has an EHR policy initiative, only 7 EU member states are routinely using EHRs. Some member states have also changed tactics, replacing top-down centralist approaches (imposing new standards and tools on health care providers) with a more decentralist, bottoms-up approach (creating incentives and setting standards but letting the market take the lead in implementing systems).
The power of data unleashed
IT is also gradually being used by health care providers in Europe to improve clinical processes and support clinical decisions. As illustrated by the Indian cases studies, this could have a tremendous impact on efficiency. Moreover, it could also significantly improve the quality and outcomes of health care. One of the key benefits of eHealth will be the tremendous amount of data that is gathered automatically via Electronic Records and Decision Support Tools. The countries that have made most progress implementing eHealth technologies (such as Israel and the Scandinavian countries) are now beginning to put their data to use to improve health care.
Health 2.0
While eHealth may be suffering somewhat from the trough of disillusionment, a new trend is emerging that is rapidly climbing the first ascent of the hype cycle: Health 2.0. In the period that health care providers and policy makers argued about how to manage the patient data they controlled, patients have been discovering the liberating effects of the internet and social networks. Over the last two decades patients have gained, via the internet, near unlimited access to the world’s stock of medical information. A motivated ePatient (using ePatient Dave deBronkart’s terminology, referring to engaged, empowered, equipped and enabled patients) can, with some effort, become a better expert on his or her disease than the attending physician. And in recent years, patients have begun forming social networks for sharing medical information. Via online platforms like CureTogether and PatientsLikeMe, people are able to compare their symptoms with each other and share advice about treatments and medical providers. Much of this information sharing is happening in a structured way enabling data mining and research. CureTogether, for example, recently reported a link between infertility and asthma (members with infertility are 40% more likely to report asthma). Patients are being empowered with highly focused, relevant information and medical science gains too because so much additional data is becoming available. All this is placing significant pressure on health care providers to adapt to these new realities by improving patient communication and moving to a more participatory style of health care provision. While many health care providers are still arguing about eHealth strategies and implementing heavy-duty IT systems, the institutions that ‘get it’, such as Radboud University Nijmegen Medical Centre in the Netherlands (see our interview with Lucien Engelen), are taking a closer look at consumer technologies and open internet platforms that lower the threshold for patient participation.
Opportunities
So what does all this mean for innovative entrepreneurs? Where are the opportunities? Based on this summary of the key innovation trends in health care, the main opportunities are in more process-driven health care delivery business models, as is experimented with in India; in telemedicine and low cost medical devices (especially diagnostic devices), to extend the reach and accessibility of health care; in data analytics tools and services (e.g. see interview with Candace Toner of Biomatters), to tackle the flood of data coming from biotech on the one hand, and eHealth and Health 2.0 platforms on the other hand.
About Author
BRAD APEL
The Fifth Conference is an innovation platform. Our goal is to stimulate innovation and entrepreneurship around the world. We interview innovators, publish a journal, organise events and make this website.